不知道有多少人吃必妥维,但有这么一个奇怪的病例分享给大家,希望可以引起大家警觉。话不多说,让我们开始吧。
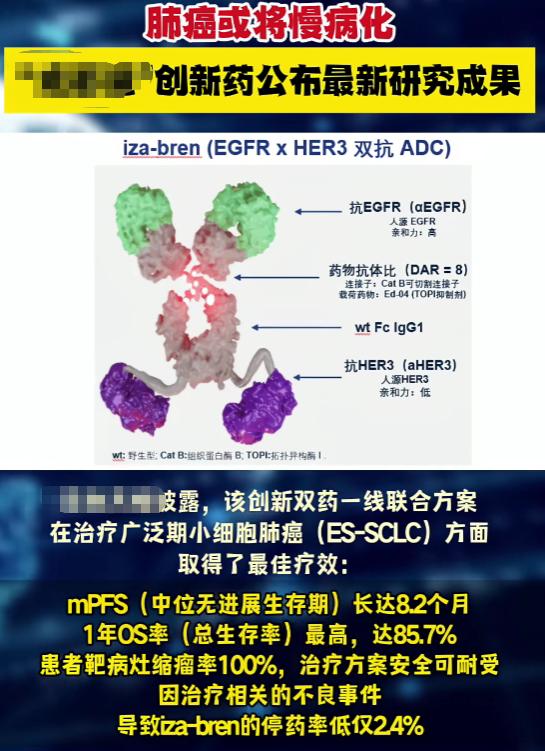
咱们都知道,必妥维(比克替拉韦/恩曲他滨/丙酚替诺福韦,也就是BIC/FTC/TAF)现在基本上是HIV治疗的一线明星药了。
它里面的BIC属于第二代整合酶抑制剂,耐药门槛相当高。临床试验里,初治患者用了它,基本没出现过整合酶耐药的情况[6,7,13]。真实世界数据更夸张——哪怕有些人吃药不太规律,或者之前就有耐药突变,都很少出问题[13]。
但2024年《Cureus》上报道的这个30岁顺性别男性,偏偏就成了那个"例外"。
他是2021年9月确诊的,基线病毒载量接近180万,CD4 335。当时做了耐药检测,NRTI、NNRTI、PI这几类老药都没发现耐药,只是没查整合酶耐药(毕竟那时候还没开始用整合酶抑制剂呢)。然后开始吃必妥维,依从性很好,病毒载量也一直压着测不到——中间2023年7月倒是停过一个月药,但恢复后很快又压下去了。

真正的转折点在2024年7月。
他突然全身不舒服、淋巴结肿大,还出现了双侧听力下降。一查,病毒载量飙到16万以上,CD4掉到328。医生一开始也懵:这人之前病毒控制得挺好,吃药也规律,怎么会突然反弹?
做了基因型耐药检测(GenoSure Prime)后,答案出来了:R263K和D67N突变。
这里得稍微解释一下这两个突变是啥意思。
R263K是整合酶抑制剂相关的一个突变,会让病毒对BIC、多替拉韦(DTG)、卡博特韦(CAB-LA)这些药的敏感性下降大概2倍。但它有个特点——会抑制拉替拉韦(RAL)耐药的发展[12]。也就是说,如果只有这一个突变,RAL反而可能成为挽救治疗的选择。这个突变以前在DTG治疗失败的患者身上见过,通常发生在依从性不好或者药物相互作用的情况下[8-10]。但在一个依从性良好的初治患者身上出现,确实挺罕见的。 理论上不能完全排除二次感染耐药毒株的可能性,虽然文献里这种情况也不多[17]。
有意思的是,R263K在体外实验里会降低病毒的复制能力和整合酶效率[11],如果再加上M184I/V突变,病毒就更"弱"了[11]。这种适应性代价,某种程度上限制了它在人群中的传播。
另一个突变D67N属于胸苷类似物突变(TAM),历史上跟齐多夫定、司他夫定这些老药有关,会降低对大多数NRTI的敏感性[18]。单独一个D67N问题不大,但如果跟其他TAM突变(M41L、K70R、L210W、T215Y/F、K219Q/E)凑在一起,就比较麻烦。特别是当有3个或以上TAM突变,而且包括M41L或L210W时,还可能产生对替诺福韦(TDF)的交叉耐药[19]。
关键来了:这个患者从来没用过胸苷类似物,却检出了D67D/N混合突变。这可能是在TDF(替诺福韦)压力下新出现的突变,也可能是极其罕见的潜伏原发性耐药。
基因型检测显示,NRTI和INSTI位点都是野生型+突变型混合毒株,这更符合继发性耐药的特点,而不是二次感染——当然,后者也不能100%排除。
顺便提一句,这位患者当时还查出了梅毒RPR滴度1:128,直肠淋球菌阳性。结合高滴度梅毒和双侧听力下降,确诊为神经性梅毒(耳梅毒),用头孢曲松治疗了14天,听力才恢复。
最后的治疗方案调整也挺有意思:从必妥维换成了Complera(恩曲他滨/利匹韦林/丙酚替诺福韦,FTC/RPV/TAF),用第二代NNRTI利匹韦林替代了整合酶抑制剂。一个月后,病毒载量重新被压下去了。

这个病例告诉我们什么?
说实话,挺让人警醒的。必妥维的耐药门槛确实高,但"高"不等于"绝对"。R263K突变即使在依从性良好的情况下也可能出现——虽然极其罕见,但它确实发生了。这也提醒我们,哪怕用着高耐药屏障的方案,定期监测病毒载量、一旦出现病毒学失败及时做耐药检测、根据结果个体化调整方案,这些基本功还是不能丢。
对了,这个患者治疗期间还合并了神经梅毒和淋球菌感染,免疫状态可能也受到了影响。虽然原文没明确说这就是耐药的原因,但多重感染确实可能让事情变得更复杂。
总之,医学里没有"绝对安全"这回事,只有"相对更安全"。这个病例就像给临床医生敲了个小警钟:即使是耐药屏障高的药,也得保持警惕。
参考文献:
Global HIV statistics — fact sheet. (2025). Accessed: February 20, 2026: https://www.unaids.org/en/resources/fact-sheet.
Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. (2025). Accessed: January 4, 2026: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent.pdf.
HIV drug resistance - brief report 2024. (2024). Accessed: February 20, 2026: https://www.who.int/publications/i/item/9789240086319.
Tsiang M, Jones GS, Goldsmith J, et al.: Antiviral activity of bictegravir (GS-9883), a novel potent HIV-1 integrase strand transfer inhibitor with an improved resistance profile. Antimicrob Agents Chemother. 2016, 60:7086-97. 10.1128/AAC.01474-16
Sax PE, Wohl D, Yin MT, et al.: Tenofovir alafenamide versus tenofovir disoproxil fumarate, coformulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: two randomised, double-blind, phase 3, non-inferiority trials. Lancet. 2015, 385:2606-15. 10.1016/s0140-6736(15)60616-x
Gallant J, Lazzarin A, Mills A, et al.: Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised controlled non-inferiority trial. Lancet. 2017, 390:2063-72. 10.1016/s0140-6736(17)32299-7
Sax PE, Rockstroh JK, Luetkemeyer AF, et al.: Switching to bictegravir, emtricitabine, and tenofovir alafenamide in virologically suppressed adults with human immunodeficiency virus. Clin Infect Dis. 2021, 73:e485-93. 10.1093/cid/ciaa988
Anstett K, Brenner B, Mesplede T, Wainberg MA: HIV drug resistance against strand transfer integrase inhibitors. Retrovirology. 2017, 14:36. 10.1186/s12977-017-0360-7
Oliveira M, Mesplède T, Quashie PK, Moïsi D, Wainberg MA: Resistance mutations against dolutegravir in HIV integrase impair the emergence of resistance against reverse transcriptase inhibitors. AIDS. 2014, 28:813-9. 10.1097/QAD.0000000000000199
Singhroy DN, Wainberg MA, Mesplède T: Combination of the R263K and M184I/V resistance substitutions against dolutegravir and lamivudine decreases HIV replicative capacity. Antimicrob Agents Chemother. 2015, 59:2882-5. 10.1128/AAC.05181-14
Quashie PK, Mesplède T, Han YS, et al.: Characterization of the R263K mutation in HIV-1 integrase that confers low-level resistance to the second-generation integrase strand transfer inhibitor dolutegravir. J Virol. 2012, 86:2696-705. 10.1128/JVI.06591-11
Wensing AM, Calvez V, Ceccherini-Silberstein F, et al.: 2025 update of the drug resistance mutations in HIV-1. Top Antivir Med. 2025, 33:457-73.
Andreatta K, D'Antoni ML, Chang S, et al.: High efficacy of bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) in Black adults in the United States, including those with pre-existing HIV resistance and suboptimal adherence. J Med Virol. 2024, 96:e29899. 10.1002/jmv.29899
Lozano AB, Chueca N, de Salazar A, et al.: Failure to bictegravir and development of resistance mutations in an antiretroviral-experienced patient. Antiviral Res. 2020, 179:104717. 10.1016/j.antiviral.2020.104717
Stoll M, Braun P, Wiesmann F, Knechten H: Development of integrase inhibitor resistance under first-line treatment with bictegravir. J Int AIDS Soc. 2020, 23 Suppl 7:e25616.
Chamberlain N, Mena L, Brock JB: Case report: emergent resistance in a treatment-naive person with human immunodeficiency virus under bictegravir-based therapy. Open Forum Infect Dis. 2021, 8:ofab297. 10.1093/ofid/ofab297
Smith DM, Wong JK, Hightower GK, et al.: HIV drug resistance acquired through superinfection. AIDS. 2005, 19:1251-6. 10.1097/01.aids.0000180095.12276.ac
Clavel F, Hance AJ: HIV drug resistance. N Engl J Med. 2004, 350:1023-35. 10.1056/NEJMra025195
Gregson J, Kaleebu P, Marconi VC, et al.: Occult HIV-1 drug resistance to thymidine analogues following failure of first-line tenofovir combined with a cytosine analogue and nevirapine or efavirenz in sub Saharan Africa: a retrospective multi-centre cohort study. Lancet Infect Dis. 2017, 17:296-304. 10.1016/s1473-3099(16)30469-8